




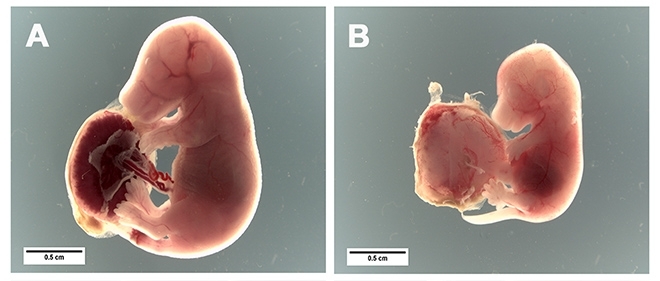
Brazilian scientists show that molecules capable of inhibiting a cell receptor known as TLR4 can prevent placental inflammation and fetal growth restriction (photos: pregnant mice were infected with the parasite that causes malaria. Fetuses developed normally in the group treated with TLR4 inhibitor [Figure A], whereas the untreated group suffered from intrauterine growth restriction [Figure B] / release)
Brazilian scientists show that molecules capable of inhibiting a cell receptor known as TLR4 can prevent placental inflammation and fetal growth restriction.
Brazilian scientists show that molecules capable of inhibiting a cell receptor known as TLR4 can prevent placental inflammation and fetal growth restriction.
Brazilian scientists show that molecules capable of inhibiting a cell receptor known as TLR4 can prevent placental inflammation and fetal growth restriction (photos: pregnant mice were infected with the parasite that causes malaria. Fetuses developed normally in the group treated with TLR4 inhibitor [Figure A], whereas the untreated group suffered from intrauterine growth restriction [Figure B] / release)
By Karina Toledo | Agência FAPESP – Infection during pregnancy by the parasite that causes malaria can not only increase the risk of a miscarriage or premature birth but also impair the fetus’s growth in the womb, so that it is more likely to die in the first few months after delivery or develop diseases in adult life.
A study conducted at the University of São Paulo’s Biomedical Science Institute (ICB-USP) in Brazil shows that all these complications of gestational malaria can be averted by preventing the activation of TLR4, a toll-like receptor found in placental cells.
Results of the research, which was supported by FAPESP, have been published in Scientific Reports.
“Intrauterine growth is restricted mainly by inflammation of the placenta, which prevents passage of adequate amounts of oxygen and nutrients to the fetus. We show that this inflammation is triggered by contact between components of the parasite and TLR4 in placental cells,” said Cláudio Marinho, a professor in ICB-USP’s Parasitology Department and principal investigator for the study.
During gestation, protozoans of the genus Plasmodium tend to accumulate in the placenta, a region with high levels of blood flow. Even after the infection has been treated with anti-parasitic drugs, the inflammation may persist until the pregnancy ends because fragments of the parasite remain deposited in tissue and may activate TLR4.
“We show that the standard treatment using anti-parasitic drugs alone isn’t sufficient to avoid complications from gestational malaria,” Marinho said. “We propose not to substitute these drugs but to add TLR4-inhibiting drugs to the therapeutic scheme.”
The strategy proved successful in tests conducted with mice at ICB-USP. Treatment with IAXO-101, an experimental drug that blocks TLR4, prevented the development of placental lesions in pregnant females infected by Plasmodium berghei and enabled them to give birth to offspring with the same average weight as the offspring of uninfected control animals.
The body weight of offspring born to infected females treated only with placebo was 20%-30% lower than that of offspring born to controls. In addition, treatment with IAXO-101 reduced maternal blood levels of TNF-α (tumor necrosis factor alpha), an inflammatory molecule considered deleterious during gestation.
Both infection and the onset of treatment with the TLR4 blocker occurred on the 13th day of gestation, equivalent to the end of the second trimester of human pregnancy. Gestation lasts 21 days in mice.
“Previous studies by our group showed that if infection occurs very early during pregnancy, the likelihood of a miscarriage is very high, and this makes testing the effects of the treatment impossible,” Marinho said.
When they administered the experimental drug to uninfected pregnant females, the researchers did not observe any difference in the weight of their offspring or in fetal development. The drug was found to be safe in all tests with mice, according to Marinho.
“No TLR4-inhibiting drugs have been approved for human use,” he said. “More studies with animals are required to guarantee the safety of a clinical trial with IAXO-101 or any other molecule that blocks TLR4.”
Trigger sought
The study was conducted during the postdoctoral research of Brazilian scientist Renato Barboza, first author of the article and currently a professor at the Federal University of São Paulo (UNIFESP).
Some of the experiments were performed at the laboratory headed by Sabrina Epiphanio, a professor in the University of São Paulo’s School of Pharmaceutical Sciences (FCF-USP), also with FAPESP’s support.
The experimental treatment was preceded by a series of tests with genetically modified mice to discover exactly which cell receptors are involved in placental inflammation.
According to Marinho, data in the scientific literature pointed to the importance of three different toll-like receptors – TLR2, TLR4 and TLR9 – in the immune response to malaria.
“Toll-like receptors act as sensors of danger and are expressed in different tissues of the body,” he said. “In the case of malaria, they’re activated by toxins known as GPIs found in the membrane of the Plasmodium parasite.”
The experiments involved three different mouse strains: one that did not express TLR2, another without TLR4, and a third without TLR9. When they were infected, only the mice lacking TLR4 failed to develop the complications typical of gestational malaria.
“Pharmacological blocking of this receptor doesn’t leave the parasite free to reproduce in the organism,” Marinho said. “Other components of the immune system continue to function normally. On the other hand, this strategy can avoid excessive inflammation, which damages both the maternal organism and the fetus.”
According to Marinho, malaria is the greatest cause of concern among parasitic diseases. Some 300 million new cases and almost half a million deaths from malaria are reported every year. About 25 million pregnant women living in countries endemic for malaria are estimated to face a heightened risk of contracting malaria and of suffering from gestational complications as a result.
“In this context, the development of new methodologies for treatment of the disease is essential,” Marinho said.
The article “TLR4-mediated placental pathology and pregnancy outcome in experimental malaria” (doi:10.1038/s41598-017-08299-x) by Renato Barboza, Flávia Afonso Lima, Aramys Silva Reis, Oscar Javier Murillo, Erika Paula Machado Peixoto, Carla Letícia Bandeira, Wesley Luzetti Fotoran, Luis Roberto Sardinha, Gerhard Wunderlich, Estela Bevilacqua, Maria Regina D’Império Lima, José Maria Alvarez, Fabio Trindade Maranhão Costa, Lígia Antunes Gonçalves, Sabrina Epiphanio and Cláudio Romerso Farias Marinho can be read at: nature.com/articles/s41598-017-08299-x.
The Agency FAPESP licenses news via Creative Commons (CC-BY-NC-ND) so that they can be republished free of charge and in a simple way by other digital or printed vehicles. Agência FAPESP must be credited as the source of the content being republished and the name of the reporter (if any) must be attributed. Using the HMTL button below allows compliance with these rules, detailed in Digital Republishing Policy FAPESP.
