




The YF virus affects the liver most of all; other organs besides the liver, however, are also affected, including the kidneys, brain, lungs, spleen, pancreas and heart (image: Erskine Palmer / CDC PHIL)
The study is the first-ever demonstration of the anatomical substrate for the cardiac arrhythmias that occur in human yellow fever.
The study is the first-ever demonstration of the anatomical substrate for the cardiac arrhythmias that occur in human yellow fever.
The YF virus affects the liver most of all; other organs besides the liver, however, are also affected, including the kidneys, brain, lungs, spleen, pancreas and heart (image: Erskine Palmer / CDC PHIL)
By Ricardo Muniz | Agência FAPESP – To fill gaps in knowledge of yellow fever (YF), a group of researchers in Brazil affiliated with the Department of Pathology at the University of São Paulo’s Medical School (FM-USP), Hospital das Clínicas (HC, the hospital complex run by FM-USP), the Heart Institute (InCor, linked to HC) and Emílio Ribas Institute of Infectious Diseases (IIER) decided to study the pathogenesis of YF-associated heart injury.
The team was led by Fernando Rabioglio Giugni, a cardiologist, and Amaro Nunes Duarte-Neto, an infectious disease specialist and pathologist; both work at FM-USP.
“There’s still no specific treatment for yellow fever. Patients receive support in intensive care, including blood transfusions, mechanical ventilation and treatment of seizures, but the death rate in severe cases is high, above 35%,” Giugni said.
The research was supported by FAPESP in the context of the Thematic Project on “The use of modern autopsy techniques to investigate human diseases (MODAU)”.
An article published recently in the journal EBioMedicine (an online open-access journal published by The Lancet Group) presents a retrospective autopsy study of cases from the 2017-19 Brazilian YF epidemic, with detailed descriptions of clinical and laboratory data, as well as macroscopic and microscopic aspects of cardiac tissue from patients who died during the period in São Paulo state. This was the worst YF epidemic reported anywhere in the world since the start of the twenty-first century, and both HC and IIER specialized in treatment of the disease at the time.
The YF virus affects the liver most of all, causing severe acute hepatitis via direct injury to hepatocytes in 5%-30% of cases. Hepatitis in YF can be fulminant, with symptoms that include nausea, vomiting, jaundice, hemorrhagic alterations (mucosal, gastrointestinal, pulmonary and cerebral bleeding), and hepatic coma.
Other organs besides the liver are also affected in YF, including the kidneys, brain, lungs, spleen, pancreas and heart. Exactly how the virus injures these organs is poorly understood. For example, YF patients are known to present with refractory hypotension (shock) and, in severe cases, with cardiac arrhythmias such as bradycardia (slow pulse), described as occurring with fever by Louisiana physician Jean Charles Faget (1818-84) in the mid-nineteenth century (and hence known as the Faget sign).
Discoveries
The main problems observed by the researchers were myocardial fibrosis and cardiomyocyte (heart muscle cell) hypertrophy in 93.2% of the cases, and (in 91.8%) alterations in the vascular endothelium, the internal lining of blood vessels, causing bleeding, edema and small blood clots in the heart. They also detected fiber necrosis in 68.5%, viral myocarditis in 12.3%, and secondary myocarditis due to bacteria and fungi in 6.8%.
The cardiac conduction system, which generates the electrical stimulus that makes the heart beat properly, was altered in 11.0%, with edema, hemorrhages and inflammation, demonstrating for the first time the anatomical substrate for the arrhythmias found in human YF.
YF viral RNA was detected in 95.7% of cases using advanced molecular biology techniques, as well as viral antigens in endothelial and inflammatory cells, pointing to direct action on heart tissue by the virus. The main inflammatory cells found in cases with myocarditis were activated macrophages.
A proteomics analysis showed higher levels of interferon gamma-induced protein 10 (IP-10, also known as CXCL-10), a chemokine produced by macrophages that attracts more inflammatory cells to the site of any injury caused by the virus. High levels of this protein were previously described in patients with COVID-19, dengue fever and Zika, and associated with a worse prognosis.
“The importance of this research is that it enables us to understand better what happens to the hearts of severe YF patients and subjects with severe reactions to the vaccine, given that the alterations in question may be masked or underestimated owing to the fulminant hepatitis typical of the disease,” Duarte-Neto said.
Myocardial injury is frequent in severe YF, owing to multifactorial mechanisms that include direct damage mediated by the virus, damage to endothelial cells, and inflammatory response (myocarditis).
“With this understanding, it’s possible to implement diagnostic and therapeutic measures to prevent and treat heart injury in YF,” he said.
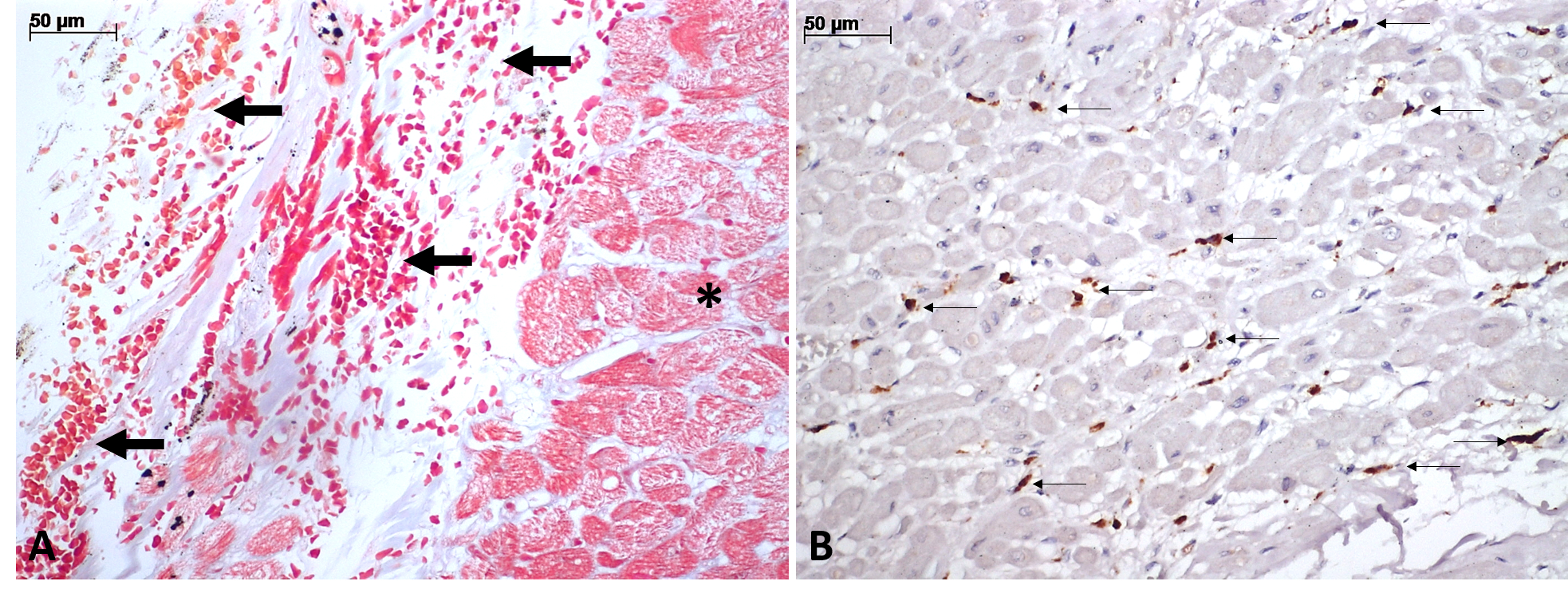
Figure A shows hemorrhage and edema (arrows) close to the cardiac conduction system (asterisk), which generates and conducts the electrical signals that coordinate contraction of the heart (stained with Masson’s trichrome). Figure B shows activated macrophages expressing the antigen CD68+ (arrows) among specialized fibers of the cardiac conduction system (immunohistochemistry). The vascular alterations (hemorrhage and edema) and inflammation (cardiac infiltration by immune cells) induced by the yellow fever virus cause arrhythmias/Image credit: Duarte-Neto & Giugni
Re-emerging disease
A total of 696 cases of YF were notified in São Paulo state between 2017 and 2019, with 232 deaths (33.3%). The main factors that contributed to establishment of the epidemic were environmental alterations, expansion of urban areas into Atlantic Rainforest remnants where circulation of the virus was increasing, and unvaccinated people going into the forest.
YF is now considered a re-emerging disease in Brazil (and Latin America generally). Vaccination is recommended throughout the country, but a substantial number of susceptible people have not received the vaccine, especially in densely populated non-endemic urban areas, which could suffer from outbreaks if the virus spreads quickly as it did in São Paulo, and indeed throughout the Southeast of Brazil, in the late 2010s.
The disease has two main forms of transmission. In the sylvatic (wild) transmission cycle, humans are infected by the bite of Haemagogus and Sabethes mosquitoes. In the urban transmission cycle, the virus is transmitted by the mosquito Aedes aegypti. The 2017-19 outbreak in São Paulo was considered an epidemic due to sylvatic transmission.
Rare cases in which complications follow vaccination are termed yellow fever vaccine-associated viscerotropic disease (YEL-AVD), typically associated with 17DD substrains of the vaccine used in South America.
The article “Understanding yellow fever-associated myocardial injury: an autopsy study” by Fernando Rabioglio Giugni, Vera Demarchi Aiello, Caroline Silverio Faria, Shahab Zaki Pour, Marielton dos Passos Cunha, Melina Valdo Giugni, Henrique Trombini Pinesi, Felipe Lourenço Ledesma, Carolina Esteves Morais, Yeh-Li Ho, Jaques Sztajnbok, Sandra de Morais Fernezlian, Luiz Fernando Ferraz da Silva, Thais Mauad, Venâncio Avancini Ferreira Alves, Paulo Hilário do Nascimento Saldiva, Leila Antonangelo, Marisa Dolhnikoff and Amaro Nunes Duarte-Neto is at: www.thelancet.com/journals/ebiom/article/PIIS2352-3964(23)00376-6/fulltext.
The Agency FAPESP licenses news via Creative Commons (CC-BY-NC-ND) so that they can be republished free of charge and in a simple way by other digital or printed vehicles. Agência FAPESP must be credited as the source of the content being republished and the name of the reporter (if any) must be attributed. Using the HMTL button below allows compliance with these rules, detailed in Digital Republishing Policy FAPESP.
